FLARE Evaluation Results
In 2007, the FLARE plan was distributed to all Michigan EDs as part of a voluntary effort to guide changes to asthma discharge instructions. Recently, the FLARE project was evaluated for impact. For this evaluation, the quality of ED asthma discharge instructions from Michigan hospitals were compared for the use of FLARE plan concepts before and after program launch. Sixty-one Michigan hospital EDs submitted discharge instructions for review with 32 EDs providing both pre and post-FLARE discharge instructions. A total of 122 discharge instructions were reviewed; 43 pre and 79 post-FLARE, with some EDs providing multiple asthma-related discharge instruction sets. Prior to review, the discharge instructions were stripped of identifying information related to the time period and institution.
Two expert reviewers scored all discharge instructions based on the follow criteria:
- Advises patient to follow up with primary doctor. (2 points)
- Advises patient to take prescribed medications as the doctor has directed. (2 points)
- Informs patients that asthma is a chronic (life-long) disease. (1 point)
- Informs patients that most people with asthma do not get so sick that they need emergency care and/or emergency asthma care may indicate treatment or management failure. (1 point)
Individual scores were then summed and averaged with a maximum total score of 6 points. A third expert provided independent review of the instructions when scores between the first and second reviewer differed significantly and when there were missing criterion scores (n=65), . If the highest and lowest of 3 scores were equidistant from the median score, the two lowest scores were averaged to determine the final score. For instructions with missing values, the review with missing data was omitted and the final score represents the average of the other two complete scores. The mean pre-FLARE review score was 3.16, the average post-FLARE review score was 3.45.
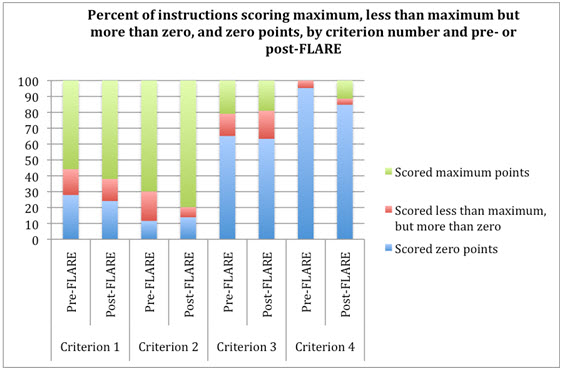
Figure 1 shows the percent of instructions awarded the range of scores (zero to full points) by criterion for the pre- and post-FLARE period.
- More ED asthma discharge instructions were awarded the maximum score post-FLARE as compared to pre-FLARE for criteria 1, 2 and 4.
- Notably, the percent of instruction sets awarded maximum points for criterion 2 increased by 10% post-FLARE. Approximately 80% of instructions were awarded full points for criterion 2 post-FLARE.
- For criterion 3 there was slight decrease (2%) in percent of instructions awarded the maximum score post-FLARE as compared to pre-FLARE.
- Criterion 4 showed the most improvement: no instruction sets were awarded maximum points pre-FLARE and 11% of instructions were awarded maximum points post-FLARE. Although there is room for improvement on this criterion as more than 80% of instructions still scored no points on this criterion post-FLARE.
Figure 1
In the subset of 32 discharge instruction sets for which we had both a pre- and post-FLARE measure, the mean of the post-FLARE scores was slightly higher than the pre-FLARE scores but the difference was not statistically significant. The greatest improvement in ED asthma discharge instructions after distribution of the FLARE plan was the addition of information stating that "Most people with asthma do not get so sick that they need emergency care" (Criterion 4). The greatest improvement in scores was observed for Criterion 2 “Advises patient to take prescribed medications as the doctor has directed” which increased by about 10% post-FLARE.
In comparison to pre-FLARE instructions, the post-FLARE instructions showed:
- 38% of EDs were not awarded maximum points for instructing patients to follow-up with their primary care physician after the ED visit (with 24% receiving zero points for its discussion)
- 14% of EDs did not advise patient to take prescribed medications as the doctor has directed
- 63% did not advise patients that asthma is a chronic disease
- 84% did not indicate that emergency asthma care may indicate treatment or management failure
In addition to numeric scoring, expert reviewers were asked to include written notes about the accuracy of information contained within each set of instructions reviewed. These comments were reviewed by a qualitative data analyst who was blinded from whether the instruction was pre- or post-FLARE. The qualitative analysis identified themes and subthemes which were organized into 5 major categories:
1) Asthma pathophysiology
a. Contains no information about pathophysiology
b. No discussion of inflammation in asthma, only discusses airway narrowing
2) Action after ED visit
a. No medication action plan
b. No follow-up with PCP
3) Medications
a. No distinction made between quick relief and long-term controller medications
b. No information about asthma medication delivery devices
c. Does not specify that inhalers and nebulizers should not be used more than every 4 hours, although sometimes more frequent use may be necessary
4) Triggers
a. No discussion of how to avoid or control triggers for asthma
b. Erroneously recommends staying indoors to control asthma
5) Reading level is too high
According the qualitative data, improvement was made in most of the categories identified (i.e. a smaller percentage of instructions lacked specific information post-FLARE as compared to pre-FLARE). In particular, there was a 28% increase in the number of EDs that included a discussion of how to avoid or control triggers for asthma. Continued improvement is needed to make a distinction between quick relief and long-term control medications, specify a timeframe for following up with a PCP and discuss how frequently medications may be used.
The criteria scoring had limited power to detect differences pre and post-FLARE due to the small sample size of EDs submitted both sets of discharge instructions. An additional limitation to these comparisons includes the fact that some hospitals use pre-packaged ED discharge instructions which would have required not only an internal decision within the hospital to change the instructions but also a request made to the discharge instruction package vendor. The primary limitation to the qualitative analysis relates to the fact that reviewers were given the option of adding notes but notes may not have been added consistently across their total set of reviews.
While there were notable improvements in the quality of discharge instructions and the inclusion of accurate asthma information after the distribution of the FLARE plan, clearly more work is needed to improve asthma discharge instructions from Michigan EDs
What can you do? Review the materials given to your patients being discharge after an asthma visit. Are they written at an appropriate reading level? Do they include accurate information, directing patients to follow-up with their primary care physician, and take their medications as directed? Do they emphasize that asthma is a chronic disease, and needs to be treated every day instead of episodically? Are you providing your patients with education about asthma self-management and consider making inhaled corticosteroids a routine prescription at discharge. The asthma information included in the FLARE plan can be used as a teaching guide at discharge and for supplemental information once home.
Adoption and implementation of the FLARE plan discharge instructions continues in Michigan EDs- most implementing hospitals have had a staff champion, and many have worked with local asthma coalitions and other partners to assist in this process. The College endorses the concept of the FLARE plan and encourages each hospital to examine, update and improve their discharge instructions for asthma. You can find the FLARE plan at getasthmahelp.org/FLARE.asp, and contact Tisa Vorce with any questions about the document or its implementation (vorcet@michigan.gov or 517.335.9463).